
Eostrogen increases throughout gestation and is very important for driving the changes as you go
into labour. Progesterone has the job of keeping the gestation going. At the end of pregnancy there is a change in the receptivity to progesterone and eostrogen will start to take over, and starts to drive changes in the uterus that induces labour. The problem when one is thinking about this from a treatment point of view is that you’re not just treating one patient, you are treating two (that are intimate), the mother and the foetus.
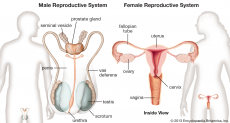
Once a placenta is established, a trophoblast of the placenta chew their way into the wall of the uterus, stripping away the outer lining of the uterine wall muscles, creating a single cell layer between the two blood interface layers, such that you can exchange gases, nutrients and hormones. There is now an intimate dialogue going on between the baby and the mum as the baby starts to develop. The signals passing through this interface are critical for how the mum interprets how well the baby is doing, and how the pregnancy matures such that you can develop a viable foetus.
As gestation increases in time, corticotrophin releasing hormone (crh) is starting to be produced in increasing quantities. crh acts on a specialised adrenal gland. When you are a foetus the adrenal gland acts differently to when you grow up, it has got a very specific purpose. One of its important purposes is that it produces the hormone cortisol. Cortisol is critical for maturing the babies key organs, for example the brain, lungs and gut. Without it, they wont develop properly.
Humans are amniotes, we have the amniotic sac, an important organ that keeps the amniotic fluid so baby can breath, keeps the environment sterile (bacterial infections that might come up the vagina/ cervix are blocked), and it is important in terms of its tensile strength. Its outer layer the amnion, the corion- fetal tissues, decidua.
In the human we have cholesterol (from plasma membrane) as the main substrate to make progesterone. We don’t have the enzymes to make estrogen in the placenta to make it directly, so cholesterol has to come from the fetal adrenal cortex, which is used to make the precursor DHEA-S, desulphated in the liver to make DHEA and converted into estrogen. This is in sort of related to how well the baby is doing, if the baby is doing well, and has a functional hp access, is increasing in size, and is maturing well, the baby will start to produce increased substrate to drive that delivery of estrogen. So we get pre labour to active labour. The cervix has completely dissolved away and pulled upwards, babies head should be engaged, the myometrium is primed and ready to push the babies head down through the birth canal and get an active delivery. But timing is crucial…
image-https://www.britannica.com/science/human-reproductive-system
0 Comment:
Be the first one to comment on this article.