
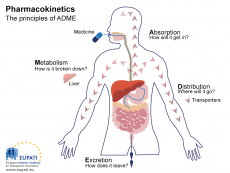
Drug metabolism goes through 2 phases. Phase 1 is where the drug molecular structure is transformed, for example through oxidation, reduction or hydrolysis. This can introduce polar groups or increase water solubility, abolish activity and can produce toxic and non-toxic metabolites. This is usually carried out by cytochrome P450 enzymes (which there are many of).
Phase 2 of drug metabolism is called conjugation. This is where an endogenous substance is attached to the phase 1 metabolite to make it more water soluble so it can be excreted in urine or bile. This is carried out by enzymes called transferases. Phase I metabolites are called primary metabolites and Phase II metabolites are called secondary metabolites.
Only unbound drug is excreted. Drugs that are lipid soluble can be absorbed in renal tubules to prolong their action. Some drugs are very dangerous if they are excreted unchanged, for example penicillin (a very famous antibiotic).
Possible routes of excretion:
Urination
Biliary into the intestine (for enterohepatic circulation- this is important for contraceptives)
Sweat, saliva, tears and expired air (but these are minor routes)
Breast milk: this is dangerous to the baby
Pharmacodynamics is concerned with how the drug interacts with the body (for example receptor sensitisation). There are various types of drugs for example: enzyme inhibitors, receptor activators, receptor blockers, enzyme false substrates, ion channel modulators and neurotransmitter uptake blockers.
What is a receptor? A protein inserted into the membrane of a cell that binds different molecules, like drugs, neurotransmitters, proteins and hormones. Binding creates a cellular response.
Different types of receptor:
G protein coupled receptors (metabotropic)
Ligand gated ion channels (ionotropic)
Kinase-linked receptors
Receptors linked to gene expression
We can measure responses to molecules binding to receptors, for example measuring muscle contraction, electrical current, change in heart rate or the production of a second messenger.
What is an agonist? A chemical that binds to a receptor and activates it. So therefore, you can guess what an antagonist is…
A chemical that binds to a receptor and inhibits its action.
Full agonists give a full response whilst partial agonists only give a partial response. We can measure how good the agonist by calculating EC50. This is the concentration of drug that gives 50% of a full response. The lower the EC50, the more potent the agonist is needed, therefore less is needed to gain a good response.
Affinity describes how well a drug binds to a receptor. Efficacy describes the drugs that bind and create a response. So, although a drug may have a high affinity, this does not mean it has high efficacy! Potency is a combination of both affinity and efficacy.
Why is there a maximum response?
There are a finite number of receptors. Therefore, increasing the drug concentration anymore will make no difference as there are no more receptors available for the drug to bind. Additionally, the properties of the tissue may limit the response. For example, the maximum muscle contraction being achieved.
For measuring ligand affinity, we cannot measure response because this involves a combination affinity and efficacy. Instead we could carry out a ligand binding assay where we use radio-labelled ligand to see how much ligand binds to receptor. However, there will be some non-specific binding that we must account for.
Image- https://www.eupati.eu/glossary/pharmacokinetics/
0 Comment:
Be the first one to comment on this article.